


April 13, 2026
What Does Mental Health Support for Men Look Like?
Explore effective men’s mental health support through integrated care, movement therapies, and peer-driven recovery by Trifecta Healthcare Institute.
Read More
Explore a step-by-step recovery plan using biohacking for addiction that enhances therapy with movement, nutrition, sleep, and breath techniques.
Start Your Journey NowWritten and reviewed by the clinical team at Trifecta Healthcare Institute, a men’s-only treatment center in Tennessee specializing in substance use, mental health, and dual diagnosis care.
Recovery from substance use disorder has a body problem. For decades, treatment leaned heavily on talk: groups, one-on-ones, step work, journaling. Those tools matter. But the brain that men bring into a treatment center has been physically rewired by alcohol, opioids, stimulants, or some combination of the three. Talking to that brain without also feeding it new physical signals leaves a lot on the table.
This section sets up why physical inputs—cold, movement, sleep, food, breath—deserve a seat at the clinical table, and what the research actually says when the wellness-influencer noise gets stripped away.
The word "biohacking" carries baggage. It conjures Silicon Valley founders microdosing nootropics and tracking heart-rate variability between Zoom calls. That framing does not serve men in recovery, and it does not serve the clinicians treating them.
A more honest definition: biohacking is the deliberate use of physical inputs to shift brain chemistry in a chosen direction. Substances did this destructively. Recovery does it constructively. Same lever, opposite outcome.
For men entering Nashville rehab or Knoxville rehab for men, that reframe matters. Cold plunges, boxing rounds, ruck hikes, and structured sleep are not extras tacked onto "real" treatment. They are how the nervous system relearns how to regulate without a substance running the controls.
The brotherhood piece is what separates this from a solo morning routine pulled off a podcast. Men recover faster when other men are in the gym, on the mat, and in the cold tub with them. Accountability stops being a worksheet and becomes a training partner who notices when someone skips a session.
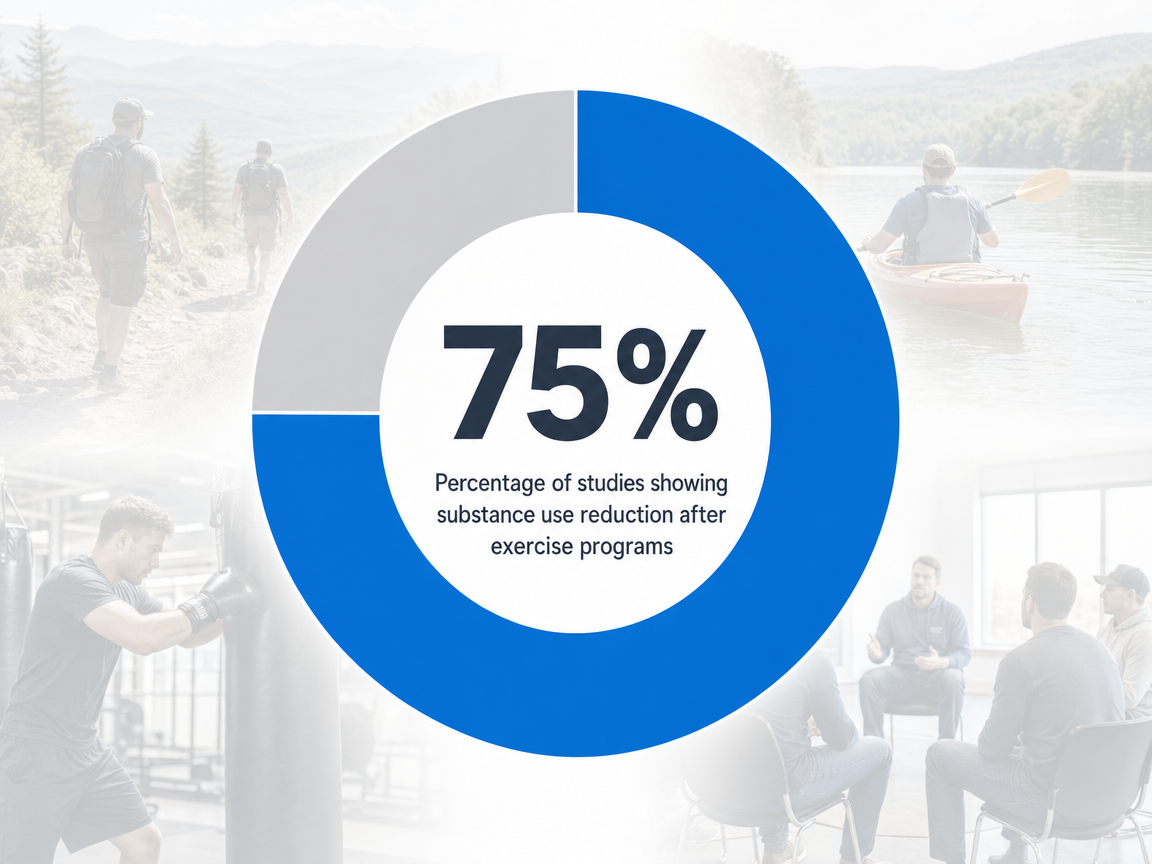
The evidence base for physical interventions in substance use disorder treatment is stronger than most people assume. A 2023 meta-analysis pooled 43 studies covering 3,135 participants across multiple substance use populations. Across studies measuring cessation or reduction of substance use, 75% reported a decrease following a physical activity intervention. Aerobic capacity improved in roughly 71% of studies that tracked it, and depression symptoms dropped in about 28% 1. The most consistent results came from moderate-intensity exercise, about one hour, three times a week, run over roughly 13 weeks 1.
That is not a wellness claim. That is a structured-protocol finding from peer-reviewed clinical research.
A separate systematic review reached the same conclusion through a different lens, finding that physical exercise positively contributes to SUD treatment by improving mental health and quality of life 10. Preclinical work fills in the mechanism: exercise activates dopamine pathways and drives neuroplastic changes in the same brain regions disrupted by addiction 16.
The legitimacy debate is over. The remaining question is how to sequence these inputs—cold, movement, sleep, food, breath, stillness—into a protocol a man can actually follow while working through clinical care.
Substances do their damage through specific channels: dopamine surges, suppressed cortisol responses, hijacked sleep architecture, gutted micronutrient stores. Recovery uses the same channels in reverse. The six inputs below—cold, movement, sleep, nutrition, breath, and stillness—each push on a particular part of the system. Used together, they give a man's nervous system more reasons to regulate itself than to chase a substance.
Cold is the fastest neurochemical tool in the recovery kit. A two- to three-minute plunge in 50-degree water raises dopamine availability for roughly 30 to 90 minutes, which is exactly the window when an acute craving usually peaks and breaks 12. The mechanism is not mysterious. Cold activates noradrenergic and dopaminergic pathways, the same circuits a substance lit up artificially.
For men in early recovery, the practical use is simple. When a craving hits hard at 7:00 a.m. or 7:00 p.m., a cold shower or plunge gives the brain a strong, legal, controllable hit of the neurotransmitters it is screaming for. The craving does not disappear. It softens enough to make the next decision a clean one.
Tennessee programs lean into this for a reason. Ice baths after a boxing round or before group therapy are not theater. They are a paced exposure to discomfort that men learn to choose, instead of running from. That choice—stepping into something hard on purpose—is the same skill needed to stay sober on a Friday night.
Safety matters. Men with cardiac conditions, uncontrolled hypertension, or active withdrawal complications need clinical clearance before plunging. Two minutes is plenty. More is not better.
Exercise is the most studied physical input in addiction medicine, and combat sports add something a treadmill cannot. Preclinical research shows that physical activity reduces drug-seeking behavior by activating dopamine pathways and driving neuroplastic changes in the exact brain regions damaged by chronic substance use 16. The reward circuit relearns how to fire on something other than alcohol or opioids.
Boxing and Brazilian jiu-jitsu work harder than steady-state cardio for two reasons. First, they demand full attention. A man rolling on the mat cannot ruminate about the bottle in his apartment because he is busy not getting submitted. Second, they involve another man. A training partner sees when someone is off, when they skipped breakfast, when something is wrong at home. That is harder to fake than checking in at a meeting.
CrossFit serves a similar function in Knoxville rehab for men—structured intensity in a group setting with names called out and rounds counted. The brotherhood is built into the workout, not bolted on after.
The dose that shows up most consistently in the research is moderate-intensity work, about an hour, three times per week 1. That is not a punishing schedule. It is a baseline that a man in PHP or IOP can actually keep, and it is enough to start moving the neurochemistry in the right direction.
Sleep is where most early recovery plans quietly fall apart. Substances damage sleep architecture, and the damage outlasts the substance. Acute drug exposure disrupts sleep latency, duration, and quality. With chronic use, the disruption gets worse, and during abstinence, insomnia and negative affect prevail—which then drives craving, impulsivity, and relapse 4. Persistent sleep disturbance after drug exposure also disrupts glutamatergic, dopaminergic, and peptidergic systems inside reward circuitry, which is a clinical way of saying poor sleep keeps the addicted brain stuck 3.
This is not a wellness preference. Sleep disturbance has been identified as a universal risk factor for relapse in alcohol use disorder 5. And current addiction medications, including those for opioid, alcohol, and nicotine use disorders, do not reverse the underlying sleep dysfunction 4. That gap is exactly where structured sleep work earns its place.
The protocol is not exotic. Same wake time every day, including weekends. Light in the eyes within 30 minutes of waking. No screens for the last hour before bed. Caffeine cut by 2:00 p.m. Room cold and dark. Men who hold this line for two weeks usually report sharper mood, fewer 3:00 a.m. cravings, and a quieter mind during group.
A man entering treatment is usually undernourished, even if he does not look it. Alcohol depletes thiamine, folate, magnesium, and zinc. Stimulants suppress appetite for weeks at a stretch. Opioids slow the gut and warp hunger cues. The result is a brain trying to rebuild dopamine, serotonin, and GABA without the raw materials it needs 17.
The research on fixing this is encouraging. A study cited in a recent review of nutrition and alcohol use disorder found that nutrition therapy combined with counseling produced reduced craving, higher nutrient intake, and greater abstinence than traditional therapy alone 6. That is a meaningful gap, and it comes from feeding men real food while they do the clinical work.
The practical version is unglamorous. Three meals a day with protein at each one. Complex carbohydrates instead of soda and candy, which dominate early recovery for the dopamine bump alone. A wellness policy study in SUD facilities found that nutrition counseling predicted lower sugar-sweetened beverage consumption, which matters because sugar swings drive mood swings drive cravings 7.
Ketogenic protocols are getting attention for stimulant and opioid recovery on the theory that ketosis supports dopamine production and lowers inflammation 14. The evidence is early. Most men do not need keto. They need breakfast.
Cravings are physical events. The chest tightens, the heart speeds up, the gut clenches. Breathwork meets the craving in the body before the brain has time to construct a story around it. Box breathing—four seconds in, four seconds hold, four seconds out, four seconds hold—and similar mindfulness practices can reduce acute craving intensity by 50 to 70 percent within five to ten minutes by shifting the nervous system out of sympathetic overdrive 15. That is a tool a man can use in a parking lot, in a bathroom stall, or in the cab of a truck.
The longer-form version is Mindfulness-Based Relapse Prevention, an eight-week structured program that grew out of Marlatt's relapse prevention work and mindfulness-based stress reduction 8. In a pilot RCT of 168 participants, MBRP participants reported an average of 2.1 substance use days at the two-month follow-up, compared with 5.4 days in treatment as usual 2. The same study noted that the gap narrowed by the four-month follow-up, which underscores why mindfulness has to be a continuing practice, not an eight-week certificate.

For men in Nashville rehab who roll their eyes at the word meditation, the framing matters. This is not incense. It is craving control with a stopwatch.
Most biohacking content treats every reader the same: morning sunlight, cold plunge, fasted training, repeat. That template breaks down inside actual recovery, where a man in detox week one and a man eight weeks into IOP are working with different bodies and different risks. The protocol below moves in stages. Each block builds on the one before it, and intensity rises only when the nervous system can handle it.
The first week is not the time for ice baths or sparring rounds. Withdrawal puts the cardiovascular system, electrolytes, and sleep architecture under real strain. The job in week one is smaller and more important: keep the body moving gently and start repairing sleep.
Walking is the main lift. Two short walks a day, twenty to thirty minutes each, ideally outside. Morning light hits the eyes within the first half-hour of waking, which begins resetting the circadian rhythm that substances spent months scrambling. Evening walks lower the cortisol load before bed.
Sleep hygiene starts now, not later. Same wake time every day. No screens in the last hour. Room cold and dark. The point is not perfection. The point is to start signaling to a brain that has forgotten what a normal sleep cycle feels like that one is on the way back.
This matters because sleep disturbance is a universal relapse risk in alcohol use disorder, and current addiction medications do not fix it 54. Walking and sleep discipline are the two interventions a man can run while his body is still finding ground.
Once detox is behind him and PHP rhythm is in place, the protocol gets sharper. This is where most of the neurochemical work happens.
Cold exposure goes in first because it is the fastest tool for managing acute cravings. A two- to three-minute cold shower or plunge raises dopamine availability for roughly 30 to 90 minutes 12. Men start with cold finishes on a regular shower, then graduate to a plunge two or three times a week. The point is not to suffer. It is to learn that discomfort is survivable and chosen.
Box breathing comes next, because cravings rarely wait for a plunge to be available. Four seconds in, four hold, four out, four hold, repeated for five to ten minutes, can drop acute craving intensity by 50 to 70 percent by pulling the nervous system out of sympathetic overdrive 15. A man can run this in a parking lot before a meeting or in the truck before walking into a hard family dinner.

Combat sports enter around week three. Boxing two days a week, jiu-jitsu one day. Moderate-intensity work, about an hour per session, three sessions weekly, is the dose that shows up most consistently in the meta-analytic data on exercise and substance use 1. The training partner is the engine. Skipping shows up faster on the mat than in a journal.
By the back half of the twelve weeks, the body has rebuilt enough capacity to handle longer, harder days. The work shifts from clinical-facility intensity toward the kind of training a man will keep doing after discharge.
This is where Tennessee terrain earns its place in the protocol. Ruck hikes in the Smokies, longer trail days along the Cumberland, ropes courses, and white-water trips ask more of the body and the group than a gym session does. Six men carrying packs up a ridge for four hours have to talk to each other, share water, slow down for whoever is struggling. The brotherhood stops being an idea and becomes something a man can feel in his hamstrings.
Strength training stabilizes around three sessions a week, combat sports continue, and cold exposure and breathwork become daily habits rather than scheduled events. Sleep targets stay non-negotiable.
The other shift is social. Knoxville rehab for men and Nashville rehab programs that run alumni programming use this stretch to introduce IOP graduates to the alumni cohort. New men see what a year of recovery looks like in a body. Older men see who is coming up behind them. That handoff is what keeps the protocol going after week twelve, when no one is checking attendance anymore.
Not every man reading this lives near a facility with ice baths and a boxing gym. The protocol still works, but the substitutions need to be honest.
Cold showers replace plunges. A pull-up bar, a kettlebell, and a pair of running shoes cover most of the strength and conditioning work for the first six weeks. Free apps run guided box breathing. State and county parks substitute for the Smokies.
The harder gap to fill is the brotherhood piece. Solo cold showers and solo runs do not carry the same accountability weight as a training partner who notices a missed session. Recovery meetings, men's groups at a local gym, jiu-jitsu fundamentals classes, and alumni programs from a prior treatment episode are where that piece comes from. A man without a clinical program nearby should call the SAMHSA helpline at 1-800-662-HELP for local treatment and peer-support referrals before building a solo plan 9.
Biohacking only earns its keep when it sits next to clinical work, not in front of it. The protocols above are not a substitute for medical detox, masters-level therapy, or medication management. They are what makes the clinical work stick.
Consider how the pieces fit. A man in DBT is learning distress tolerance—how to stay in a hard feeling without acting on it. A two-minute cold plunge is distress tolerance with a timer. He practices the skill in the tub on Tuesday and uses the same nervous-system pathway when his ex calls on Saturday. The therapist gives him the framework. The cold gives him the reps.
EMDR runs on a similar principle. Trauma processing leaves men physiologically activated, sometimes for hours after a session. Boxing rounds and jiu-jitsu rolls give that activation somewhere to go. The body discharges what the brain just opened. Several men report sleeping better the night of an EMDR session when the day includes a hard physical block, which matters because sleep dysfunction is itself a relapse risk that current addiction medications do not address 4.
Medication management benefits too. Naltrexone, buprenorphine, and acamprosate work better in a body that is sleeping, eating protein, and moving. Nutrition therapy combined with counseling has been shown to reduce alcohol craving and improve abstinence rates compared to counseling alone 6, which suggests that what a man eats during medication-assisted treatment is part of the treatment.
Mindfulness-Based Relapse Prevention illustrates the integration most clearly. MBRP grew directly out of Marlatt and Gordon's cognitive-behavioral relapse prevention model, layered with mindfulness-based stress reduction 8. It is not a parallel track to CBT. It is CBT with a body added.
The order matters. Clinical care is the spine. Movement, cold, sleep, breath, and nutrition are the muscles that hold the spine upright. Tennessee addiction treatment programs that build the protocol this way—clinicians and coaches in the same building, talking to each other—give men a recovery that does not collapse the week after discharge.
A scope note before this section develops: the audience here shifts from men working their own recovery to the masters-level clinicians, program directors, and medical staff designing protocols around them. The operational question is how to integrate physical inputs without diluting the clinical spine.
Three design choices show up consistently in programs that make this work. First, treat movement, sleep, and nutrition as scheduled clinical hours, not free-time activities. A wellness policy intervention in SUD facilities measurably increased nutrition counseling receipt and predicted lower sugar-sweetened beverage consumption among patients 7. Policy moves behavior; optional programming does not.
Second, stage intensity to acuity. Detox patients walk and rebuild sleep. PHP adds cold exposure and combat sports under supervision. IOP and alumni programming carry the load into outdoor adventure and longer training blocks. The meta-analytic dose—about an hour, three times weekly, sustained over roughly 13 weeks—is a defensible floor for IOP-stage exercise prescriptions 1.
Third, build clinician-coach communication into the schedule. When a man's EMDR therapist knows he had a hard roll on the mat that morning, and his strength coach knows he is two days post-trauma processing, the protocol stops being two parallel programs and becomes one. That coordination is what Tennessee addiction treatment programs running brotherhood-based models are operationalizing, and it is what separates integrated care from amenity stacking.
The first month decides whether the protocol becomes a life or a phase. Men who treat the early weeks as a training block, not an experiment, tend to keep going.
The shortlist for day one through thirty: pick a wake time and hold it. Walk twice a day. Eat protein at every meal. Run a five-minute box breathing set when a craving lands. Add a cold finish to the morning shower by week two. Find one other man who knows the schedule and will notice an absence.
That is the floor. Combat sports, plunges, and Smokies hikes come next, layered in alongside clinical work in PHP, IOP, or alumni programming. Men who need help building the clinical spine can call SAMHSA's National Helpline at 1-800-662-HELP, free and confidential, 24 hours a day 9.
The body is part of the treatment plan. Start there, and the rest of recovery has something solid to stand on.
The honest answer is not yet. A recent literature review suggests dopamine fasting may prove useful for people with addictive behaviors and obsessive-compulsive patterns, but the evidence base is thin and mostly theoretical 11. Cutting back on phone scrolling, pornography, and junk food during early recovery is reasonable. Calling it a proven clinical intervention is not. Treat it as a habit cleanup, not a treatment.
No. Naltrexone, buprenorphine, and acamprosate have decades of evidence behind them. Cold plunges and boxing rounds do not replace that. They make it work better. Nutrition therapy paired with counseling produced reduced cravings and higher abstinence than counseling alone 6, which is the right framing—physical inputs amplify clinical care. Men in medication-assisted treatment should keep taking their medication and add the protocol around it.
Anyone with a cardiac condition, uncontrolled hypertension, a seizure history, or active withdrawal complications needs medical clearance before plunging. Cold drives a noradrenergic spike that the heart and vasculature have to absorb 12. Pregnant women and men with Raynaud's also sit this one out. The fix is not skipping cold work entirely. Cold-finish showers, 30 to 60 seconds, give most of the benefit at a fraction of the load.
Different inputs work on different clocks. Box breathing can drop acute craving intensity by 50 to 70 percent within five to ten minutes 15. Cold raises dopamine for 30 to 90 minutes 12. Sleep discipline shows up in mood and cravings inside two weeks. The exercise meta-analysis found the most consistent substance-use reduction at roughly 13 weeks of moderate-intensity training, three times weekly 1. Stack the timelines.
Solo routines collapse on hard days. A training partner does not. Men who roll on the mat together, lift together, and hike together build accountability into the schedule rather than relying on willpower. The protocol is the same. The follow-through is different. Knoxville rehab for men and Nashville rehab programs that build cohorts around movement see this play out—men who skip a session get a text from another man, not from staff.
SAMHSA's National Helpline is free, confidential, and runs 24 hours a day, 365 days a year, in English and Spanish, at 1-800-662-HELP (4357) 9. The line connects callers to local treatment, peer support, and family resources. For men in Tennessee specifically, programs offering medical detox, PHP, and IOP with movement-based programming are available in the Nashville and Knoxville areas. Call before building a solo plan.
April 13, 2026

April 15, 2026

April 15, 2026