


April 13, 2026
What Does Mental Health Support for Men Look Like?
Explore effective men’s mental health support through integrated care, movement therapies, and peer-driven recovery by Trifecta Healthcare Institute.
Read More
Explore how brotherhood after rehab strengthens lasting sobriety through peer support, structured aftercare, and rebuilding social connections.
Start Your Journey NowWritten and reviewed by the clinical team at Trifecta Healthcare Institute, a men’s-only treatment center in Tennessee specializing in substance use, mental health, and dual diagnosis care.
The day a man walks out of a residential program, his clinical schedule disappears, but his nervous system still expects the people, places, and routines that fed his substance use. That gap between what treatment built and what daily life actually offers is where most relapses begin. Brotherhood after rehab is the practical answer to that gap, and the research on why it works is more specific than the usual aftercare pep talk suggests.
Two ideas explain most of what brotherhood actually does for a man in early recovery: abstinence self-efficacy and group cohesion. Self-efficacy is the belief that he can stay sober in a specific situation — a Friday night, a fight with his partner, a layoff — and it climbs when other men around him model that it is possible. Researchers studying social networks in substance use recovery have found a clear positive relationship between general social support and abstinence-specific self-efficacy, meaning the more credible support a man has around him, the more he believes he can hold the line under pressure 2.
Cohesion is the second piece. In group therapy and peer settings, cohesion describes how tightly members listen to each other, take each other's recovery goals seriously, and hold the room together when things get hard. Studies on group dynamics in SUD treatment show that when members actively support one another's recovery goals, cohesion improves and so do outcomes 5. That is not a soft finding. Cohesion is what turns a roster of strangers into a group a man will actually call at 11 p.m. instead of driving past the liquor store.
For men leaving Nashville rehab or a Knoxville rehab program, the mechanism matters because it tells him what to look for. Not motivational quotes. Not the loudest voice in the room. He needs a small group of men whose own behavior reinforces his belief that staying sober is possible, and who will keep showing up consistently enough that the group itself feels stable.
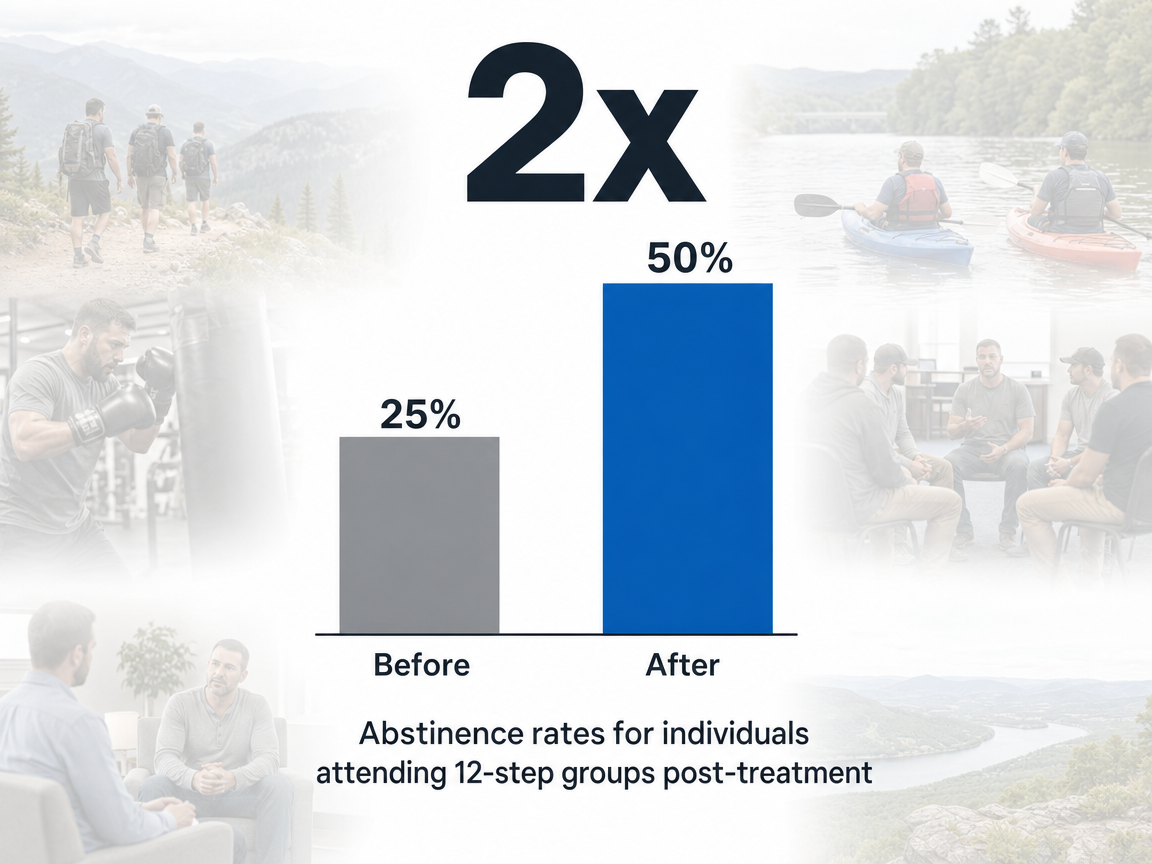
The most cited finding in this space comes from a longitudinal study of men receiving inpatient care through the Veterans Affairs system. Among that population, abstinence rates were roughly twice as high for men who attended a 12-step group like Alcoholics Anonymous after discharge compared with men who did not, and the relationship was almost linear with meeting frequency — more meetings, better outcomes, in a near dose-response pattern 3. The scope is worth naming directly: this was a male VA sample coming out of inpatient treatment, not a universal guarantee for every man in every program. Even so, it remains one of the cleanest signals that structured peer attendance changes the math of staying sober.
The peer recovery coaching literature points in the same direction with a different design. A systematic review of randomized trials examining peer recovery support services found a roughly 14% reduction in alcohol and other drug use in coached groups compared with a roughly 15% increase among controls over the follow-up window 4. The two findings come from different methods and different populations, but they converge on a practical point: structured peer connection after treatment shifts behavior in a measurable way that solo aftercare rarely matches.
A 2025 systematic review of peer recovery support services adds retention to the picture, finding that peer-delivered services contribute to reductions in substance use and relapse rates while improving how long people stay engaged with recovery resources 12. Retention matters because the men who quietly drift out of aftercare are the ones who are hardest to track and easiest to lose.
Numbers like these do not promise anything to any individual man. They describe what tends to happen across groups of men who build a peer-supported life after discharge versus those who do not. For a man weighing whether to treat brotherhood as optional, that is the relevant frame.
Most discharge plans hand a man a list: a therapist's number, a meeting schedule, maybe a recovery coach if he asks. What that list cannot do is replace the social architecture his substance use built over years. The exposure starts the week he gets home.
The first thirty to ninety days after discharge are when the structure of treatment thins out fastest. PHP ends. IOP tapers. The man who saw clinicians and peers five days a week is suddenly seeing them once a week, then twice a month, then on his own initiative. That tapering is clinically appropriate, but it leaves a vacuum where the using network used to live, and the new sober network has not yet formed.
Research on social support in recovery populations consistently links the size and quality of a man's post-treatment network to his substance use outcomes. Greater social support has predicted lower substance use rates after treatment, with residents of recovery homes who maintain high mutual-help participation more likely to hold long-term sobriety 1. The inverse is the warning: a man who leaves treatment and goes home to the same phone contacts, the same coworkers at the same bar after shift, the same Saturday routine, is rebuilding nothing. He is renting sobriety from his willpower until the willpower runs out.
SAMHSA's work on reentry and community integration names this directly. Peers provide a sense of belonging and supportive relationships that bridge the gap between formal treatment and ordinary life 14. For a man leaving a Nashville rehab program or returning home from Knoxville rehab for men, that bridge has to be built before he needs it, not after the first hard Friday night. The aftercare cliff is real, and it is mostly a social problem.
Two kinds of social capital tend to matter in recovery, and standard aftercare often supplies neither cleanly. Bonding capital is the deep, repeat-contact tie inside a small recovery group — the men a guy texts when he is rattled, the ones who notice when he stops showing up. Linking capital is the wider web of sober contacts that opens doors: a job lead, a sponsor's friend, a Saturday hike with people he barely knows yet but who do not drink. Both protect sobriety in different ways. A weekly meeting alone usually builds neither at sufficient depth.

The honest caveat belongs here. A systematic review of nine studies on peer-delivered recovery support services concluded that the body of evidence suggests salutary effects on substance use and recovery factors, while flagging significant methodological limitations across the studies — small samples, varied designs, and mixed control conditions 11. Translation: peer support reliably looks like it helps, and it almost certainly does, but the field has not yet produced the kind of large, tightly controlled trials that would let anyone claim a precise effect size.
That ambiguity is a feature of the conversation, not a reason to dismiss it. The signal across studies points the same direction. What the limits mean for a man planning his aftercare is straightforward: the evidence supports building a structured peer network as a core layer of recovery, not a polite afterthought, while staying skeptical of any program that promises a specific percentage of relapse reduction as if the number came from a settled science.
The word brotherhood gets thrown around in recovery marketing without much definition. In practice, a functional brotherhood after rehab has a few specific traits: it holds a man accountable without humiliating him, it gives his identity somewhere to land that does not involve substances, and it works whether or not he loves every person in the room. The next three sections describe how that actually takes shape.
Accountability is the part most men say they want and most men quietly resent when it arrives. The version that works in early recovery is not a friend nagging him about his step count or a sponsor checking his receipts. It is another man who has been through the same kind of collapse, who can ask a direct question without flinching, and who is not trying to fix him.
SAMHSA's framing of peer support workers names this dynamic clearly: peers who share lived experience help people stay engaged in recovery and reduce the likelihood of relapse, largely because their credibility is earned rather than credentialed 7. A man in his first ninety days will accept a hard question from someone who has sat in the same chair. He often will not accept it from a clinician, a parent, or a partner, even when the question is identical.
The research on group cohesion adds the second piece. When members of a recovery group actively support one another's goals — listening without rushing to advice, showing up when they said they would, naming what they see without contempt — cohesion improves and outcomes follow 5. Shame does the opposite. A group that polices each other through guilt produces compliance for a few weeks and dropouts after that.
For men in a Nashville rehab program or stepping down from Knoxville rehab, the practical version looks small: a peer recovery coach who texts on Tuesday mornings, a brotherhood cohort that meets after a Wednesday workout, a sponsor who picks up on the second ring. The accountability is high. The judgment is low. That combination is what keeps a man in the room long enough for the other parts of recovery to take hold.
Most men leaving treatment have a quiet question they rarely say out loud: who am I now if I am not the guy who drinks, uses, or numbs? Talk-only aftercare can address that question slowly. Shared physical work tends to address it faster, because identity rebuilds through what a man does with his body alongside other men, not just through what he says about himself in a circle of chairs.
The cleanest data point on how quickly a sober identity can take hold comes from a study tracking residents in recovery homes. Within the first six months, residents shifted to social networks that were 100% sober, and median abstinence self-efficacy — the belief that staying sober is possible under pressure — rose by nearly 10 points 6. The takeaway is not that every man needs a recovery home. It is that immersive sober environments can rewrite a social network and a self-concept inside half a year, which is faster than most men assume is possible when they walk out of detox.
Movement-based programming compresses some of the same effect into shorter windows. When men show up for jiu-jitsu rolls, boxing rounds, ice baths, or a hike up a Tennessee ridge, the cohesion researchers describe in group therapy gets built through a different door. A man who has been choked out and helped up by the same training partner three times a week stops performing recovery and starts living inside it. The body learns that effort, fatigue, and discomfort can be metabolized in a room full of sober men instead of a bar full of using ones.
This is the part of brotherhood that resists slogans. Identity does not rebuild through inspirational language. It rebuilds through repetitions: the same parking lot, the same warm-up, the same group of guys nodding at each other before the first round. Over months, a man stops being the person he was when he arrived and becomes the person his current behavior describes. For programs at Trifecta's Spring Hill and Knoxville facilities, that is the function physical programming serves — not entertainment, not novelty, but a structured way to keep men working shoulder to shoulder until the new identity feels less like a costume and more like a fact.
The fair question to ask about a men's-specific program is whether the gender split actually matters or whether it is just marketing. The honest answer is that the evidence is mixed in a way most brochures do not admit. A study comparing men's and women's experiences in group therapy for substance use disorders found that men more frequently endorsed the helpfulness of mixed-gender groups, while women more often preferred single-gender ones 9. That finding alone could be read as an argument against men's-only programming.
The better reading is that group composition is one variable among several, and the case for a men's brotherhood does not rest on men disliking mixed groups. It rests on the specific work that happens when men in recovery sit with other men around shared masculinity scripts, shame patterns, fatherhood, work identity, and the particular ways men tend to isolate. Those conversations move faster and deeper in a room of men than in a mixed setting, even when the men in question would have rated a mixed group as helpful on a survey.
A men's-only brotherhood is not a claim that mixed groups fail. It is a claim that some of the work in early recovery — anger, sexual shame, father wounds, the performance of competence — gets addressed more directly when the room is built for it. That is the case Tennessee men's programs earn or do not earn through what actually happens inside the room.
The standard discharge advice — find a sponsor, attend meetings, call your therapist if things get hard — treats aftercare like a single line item. A more useful frame is a stack: five layers, each doing different work, each with its own weekly time cost. When one layer thins out, the others hold. When a man tries to run on one layer alone, the structure collapses the first time pressure hits.
The layers, in order of clinical intensity, look like this. Clinical care comes first: a therapist or psychiatrist who manages the work that requires a credential, including co-occurring depression, anxiety, or trauma alongside the substance use disorder. For most men in the first six months after PHP or IOP, this is one to two hours a week. A peer recovery coach sits next — a trained worker with lived experience who texts on a known cadence, helps with logistics, and bridges the gap between clinical sessions. SAMHSA describes peer workers as a layer that helps people stay engaged in recovery and reduces relapse likelihood through shared experience 7. Plan on thirty minutes to an hour weekly, sometimes more in early months.
The brotherhood cohort is the third layer and the one most men underweight. This is the small, stable group of men a guy sees in person on a recurring schedule — a Wednesday meeting, a Saturday workout, a Tuesday dinner — where cohesion has time to form because the same faces keep showing up. Two to four hours a week is a realistic floor. The fourth layer is family and partner support: structured conversations with a spouse, a parent, or close friend who understands the recovery framework rather than guessing at it. NIAAA's guidance treats mutual-support participation as an added layer that helps sustain beneficial changes, and the same logic applies to the people inside a man's home 8. Time cost varies, but a weekly check-in is the minimum that tends to work.
The fifth layer is the movement community — the gym, the jiu-jitsu academy, the hiking group, the boxing class. It is not therapy, and it does not pretend to be. It is the place identity rebuilds through shared physical work alongside men who are not using. For programs like Trifecta's in Spring Hill and Knoxville, this layer is built directly into the clinical model so men leave treatment already inside a movement community rather than searching for one. Three to five hours a week is typical.
Why stack rather than substitute? A 2025 systematic review of peer recovery support services found that PRSS contribute to reductions in substance use and relapse rates while improving treatment retention — meaning men stay engaged with recovery resources longer when peer layers are present 12. Retention is the quiet variable. The man who keeps showing up to three layers in month nine is the man who is still sober in year two. The stack is what keeps him showing up.
Brotherhood after rehab can fail in ways that look fine on the surface for months before the cracks show. Three patterns account for most of the trouble.
The first is the codependent dyad. Two men in early recovery latch onto each other so tightly that the rest of the network thins out. They text constantly, rescue each other from every wobble, and stop showing up to the broader group because the pair feels like enough. When one of them slips, the other usually goes with him. The protective effect of a sober network depends on its breadth, not just its intensity — the recovery home research showing rapid shifts to fully sober social ties within six months describes a network, not a partner 6. A man should be able to name five or six guys he would call before midnight, not one.
The second is brotherhood as performance. The meetings get attended, the right phrases get said, the workouts get posted, and underneath it the man is white-knuckling alone. Group cohesion research is clear that outcomes improve when members actually support each other's goals rather than going through motions 5. Performance is the opposite of cohesion. It is what a man does when he is afraid to be honest about a craving, a fight at home, or the fact that he has been thinking about using for two weeks.
The third is the slow drift after PHP or IOP ends. Attendance at the brotherhood cohort goes from weekly to twice a month to whenever. The peer coach calls go unanswered. Nothing dramatic happens — until it does. SAMHSA's framing on peer workers names the function being lost: shared-experience contact that keeps men engaged in recovery and reduces relapse likelihood 7. The drift is the most common failure mode because it does not feel like a failure. It feels like getting busy. The fix is to treat the schedule as non-negotiable for the first eighteen months, the way a man treats a medication he cannot afford to skip.
Sobriety that lasts is not built on willpower or a perfect morning routine. It is built on who a man sits next to on Wednesday nights, who picks up the phone on Saturday afternoon, and who he trains alongside until effort and discomfort stop sending him toward a drink. Brotherhood after rehab is the work of replacing one social operating system with another, and the evidence supports treating it as core, not optional. For men finishing care at Trifecta's Spring Hill or Knoxville facilities, the brotherhood already exists by the time discharge arrives. For men leaving any other Tennessee program, the assignment is the same: build the network before the pressure comes, and keep showing up after it does.
Ideally, the first peer contact happens before discharge, not after. The riskiest window is the first thirty to ninety days, when clinical structure thins out and old social cues come back fast. A man who already has a peer recovery coach's number saved, a brotherhood cohort meeting on his calendar, and one mutual-help group he has visited at least once is far better positioned than a man assembling all of that from his couch. SAMHSA frames peer workers as a layer that keeps men engaged and reduces relapse likelihood, which only works if the connection exists before it is needed 7.
Virtual groups can carry real weight, especially for men in rural Tennessee or anywhere a drive to a meeting is an hour each way. The usual finding that mutual-support participation helps sustain the changes treatment started applies whether the room is physical or on a screen 8. The honest caveat is that screen contact tends to build cohesion more slowly than in-person work, so a man relying on virtual groups should add at least one in-person anchor — a gym, a sober hiking group, a single weekly meeting within driving distance — to round out the network.
Old ties fall into three buckets: friends who actively used with him, friends who drank around him without it being central, and friends who never had much to do with the substance. The first group has to wait, often for a year or more. The second can be tested slowly, in sober settings, after the brotherhood network is stable. The third can usually be rebuilt earlier. Research on recovery-home residents shifting to fully sober networks within six months suggests the new network needs protected room to form before old ties get reintroduced 6.
Yes. The mechanism that makes peer support work — shared experience, accountability without shame, abstinence self-efficacy built through credible models — is not exclusive to 12-step rooms. A systematic review of peer recovery support services found reductions in substance use and improved retention across a range of formats, not only AA or NA 12. SMART Recovery, peer recovery coaching, men's groups inside a treatment alumni program, and movement-based cohorts all build the same underlying network. The 12-step path is one well-mapped option, not the only one that earns a man long-term sobriety.
A few patterns show up consistently. The two men talk almost exclusively to each other and stop engaging the broader group. One rescues the other from every wobble instead of pointing him back to the network. Honesty narrows because the friendship feels too important to risk. Attendance at the wider brotherhood drops. Group cohesion research is clear that recovery outcomes improve when members support each other's goals across a network, not inside a sealed pair 5. A useful test: if a man cannot name five other guys he would call before midnight, the dyad has gotten too tight.
Brotherhood is not a substitute for clinical care of depression or anxiety, and Trifecta treats co-occurring mental health conditions alongside substance use disorder rather than as primary mental healthcare. That said, the social side of recovery does meaningful work on mood. Achieving recovery is associated with broader psychosocial improvements, including in well-being and connection 10. A man managing depression alongside SUD still needs a therapist, a psychiatrist when indicated, and possibly medication. The brotherhood layer supports that clinical work by reducing isolation, which is one of the strongest amplifiers of both relapse risk and depressive symptoms.
April 13, 2026

April 15, 2026

April 15, 2026