


April 13, 2026
What Does Mental Health Support for Men Look Like?
Explore effective men’s mental health support through integrated care, movement therapies, and peer-driven recovery by Trifecta Healthcare Institute.
Read More
Learn how to assess if short term drug rehab fits your needs and explore key factors that boost recovery success and aftercare engagement.
Start Your Journey NowWritten and reviewed by the clinical team at Trifecta Healthcare Institute, a men’s-only treatment center in Tennessee specializing in substance use, mental health, and dual diagnosis care.
As a referring professional, you know that guiding a man in crisis requires swift, decisive action. A short term drug rehab program, clinically referred to as short-term residential treatment, is an intensive, time-limited intervention typically lasting 28 to 30 days. Unlike outpatient or long-term residential models, these programs are designed to provide a safe, highly structured environment focused on acute stabilization, crisis intervention, and the initiation of recovery skills.
Facilities deliver round-the-clock support, including medical detox, evidence-based group therapy, individual counseling, and psychoeducation targeting substance use disorder (SUD) and co-occurring mental health symptoms. It is important to note that facilities like Trifecta Healthcare Institute expertly manage co-occurring mental health conditions alongside substance use, but they do not offer primary mental healthcare. Typically, a 30-day residential episode requires a time investment of 28 to 30 days and a financial investment ranging from $15,000 to $30,000, depending on the facility's medical capabilities and insurance coverage.
Within this framework, participants follow a regimented daily schedule that integrates wellness or movement-based activities. This aligns with contemporary best practices that recognize the role of physical health in early recovery. The treatment team coordinates discharge planning from the outset, emphasizing continuity of care and seamless transition to lower levels of support.
This approach works best when the primary goal is to interrupt the immediate cycle of use, address acute withdrawal, and build initial motivation for ongoing treatment. It is especially relevant for men requiring stabilization before stepping down to partial hospitalization, intensive outpatient, or sober living environments6. Short-term models remain the most widely available residential treatment format nationwide, reflecting both clinical utility and insurance reimbursement realities.
The evidence base for short-term residential programs highlights both strengths and limitations. These programs reliably address immediate stabilization, acute withdrawal, and initial engagement—making them a crucial first step for many men in crisis. According to peer-reviewed research, individuals completing short-term residential treatment see improved outcomes when they transition directly into structured continuing care, with treatment completion rates rising from 50% to 70% in these cases2.
However, the effectiveness of short-term stays declines when participants do not access robust outpatient or step-down support, underscoring the importance of integrated aftercare planning. Approximately 45-60% of those entering treatment for substance use disorder also live with a co-occurring mental health condition, further complicating placement decisions and influencing success rates3.
For men who require medical stabilization but lack severe, chronic relapse histories, this model often provides a practical and accessible entry point. Consider this method if your goal is to deliver rapid stabilization while building bridges to longer-term recovery resources. As the field moves toward individualized, assessment-driven placement, understanding the clinical indicators that guide program matching becomes increasingly important.
| SUD Severity | DSM-5-TR Criteria | Recommended Program Intensity |
|---|---|---|
| Mild | 2–3 criteria | Evaluate for intensive outpatient or short-term residential |
| Moderate | 4–5 criteria | Consider short-term residential, with strong aftercare focus |
| Severe | 6+ criteria | Prioritize extended residential or integrated step-down continuum |
Accurate severity assessment lays the foundation for treatment matching in substance use disorder care. Using standardized criteria like the DSM-5-TR provides a clear framework: mild, moderate, and severe substance use disorder. These specifiers guide clinicians in determining whether a 30-day model is appropriate or if longer, more immersive interventions are needed4.
A 30-day residential stay is ideal for men exhibiting mild to moderate SUD symptoms, particularly when there is no entrenched pattern of relapse or life-threatening withdrawal risk. This strategy suits organizations that need to provide rapid stabilization, initial skill-building, and a structured environment before moving clients to outpatient or community-based supports.
In practice, men with severe SUD—especially those with a chronic relapse history, polysubstance dependence, or medical instability—require greater intensity and duration, often in an extended residential setting. Program selection should also factor in acute safety needs, withdrawal management requirements, and readiness for aftercare. Employing validated clinical assessment tools and multidisciplinary input helps avoid premature step-down or unnecessary overtreatment2.
Thorough screening for co-occurring mental health conditions is a non-negotiable step when matching individuals to the right level of care. Research indicates that 45-60% of men seeking SUD treatment also meet criteria for a mental health diagnosis, such as depression, PTSD, or anxiety disorders3. Dual-diagnosis presentations often predict a higher risk for relapse, crisis events, and disengagement if not addressed during initial placement.
Opt for this framework when rapid stabilization alone is unlikely to address the full scope of a client’s needs. Using structured screening instruments alongside clinical interviews helps identify psychiatric comorbidities early. For example, the Patient Health Questionnaire-9 (PHQ-9) screens for depression, while the Generalized Anxiety Disorder-7 (GAD-7) is commonly used for anxiety. Incorporating these tools enables teams to flag men who may require integrated psychiatric support or modifications to the typical rehab structure.
This method is highly effective for programs serving professionals or veterans, where trauma histories and undiagnosed conditions are prevalent. Screening also supports tailored aftercare planning, as those with dual diagnoses benefit most from coordinated outpatient psychiatric follow-up3. Remember, facilities like Trifecta focus on treating these co-occurring issues in tandem with addiction, rather than acting as a primary mental health facility.
| Profile Indicator | Favorable for 30-Day Rehab |
|---|---|
| SUD Severity | Mild to moderate |
| Motivation Level | Strong external motivation (family, legal, professional) |
| Living Environment | Stable or supportive post-discharge |
| Relapse History | No recent history of severe, repeated relapse |
| Mental Health | Manageable co-occurring conditions |
A 30-day residential stay is most effective for men who present with clearly defined, time-limited needs—such as acute withdrawal, a first episode of SUD, or the necessity for crisis stabilization before returning to life responsibilities. This path makes sense for individuals with strong social support networks, employment stability, and readiness to transition quickly into continued care.
For example, professionals or veterans with mild to moderate SUD often benefit from short-term programs, provided that robust aftercare is arranged10. Predictors of positive outcomes in this setting include high motivation to change, prior successful treatment engagement, and access to ongoing outpatient services.
Conversely, men with chronic relapse patterns, severe trauma histories, or unstable housing typically require longer or more intensive care to achieve sustained recovery5. If your client’s primary obstacles are acute and can be addressed within a focused, structured timeframe, this model is highly appropriate—but always anticipate the need for seamless aftercare linkage to sustain gains.
Continuity planning is a primary determinant of long-term success. Research consistently demonstrates that treatment completion rates rise from 50% to 70% when participants move directly from residential care into structured aftercare programs, such as outpatient therapy, alumni groups, or community-based supports2.

Despite this, only about 35% of treatment centers nationally provide formal protocols that connect short-term program graduates to the next level of care, creating a significant gap in the recovery continuum6. This approach is ideal for organizations serving men whose acute stabilization needs have been addressed but who require structured guidance to maintain progress.
Effective continuity planning involves more than a referral; it means building a clear, actionable bridge to ongoing therapy, peer support, and, when necessary, psychiatric care. As the field evolves, telehealth and digital tools are increasingly used to support men after rehab, extending the benefits of face-to-face programming into daily life.
Stepped-care models offer a layered approach to recovery by matching treatment intensity to the individual’s current clinical needs and gradually adjusting as stability improves. In Tennessee, this often starts with a structured residential stay at a Nashville rehab or Knoxville rehab for men, designed to interrupt acute substance use and initiate foundational change.
Once immediate risks are managed, men can transition seamlessly into less intensive supports—such as partial hospitalization, intensive outpatient, or sober living. This allows for a progressive decrease in clinical supervision while maintaining essential recovery scaffolding. Consider this route if you aim to maximize engagement and minimize relapse risk during transition periods.
Only 35% of U.S. facilities currently offer formal stepped-care continuity, despite its demonstrated impact on long-term outcomes6. Regular reassessment ensures that men neither drop out prematurely nor remain in high-intensity care longer than necessary.
Incorporating movement-based recovery into residential care offers measurable advantages, particularly for men seeking active engagement over traditional talk therapy alone. Elements of effective movement-based programming include daily structured physical activity (e.g., boxing, jiu-jitsu, hiking), group-based movement fostering peer accountability, biohacking modalities like ice baths, and outdoor adventure therapy.
Research underscores how structured physical activity not only supports mood regulation and stress reduction, but also improves treatment retention and post-discharge engagement, especially when paired with peer group participation2. This method works when your clinical population struggles with motivation, emotional regulation, or past disengagement from sedentary programming.
By integrating movement, programs like Trifecta Healthcare Institute can accelerate neurobiological healing and reinforce the brotherhood dynamic that predicts stronger aftercare outcomes10. It provides kinesthetic learning and camaraderie that resonates deeply with veterans and professionals alike.
"Thirty days establishes the foundation—medical stability, therapeutic tools, physical resilience, and peer connections. The foundation is built. What comes next determines whether it becomes permanent."
When guiding a professional peer or client into treatment, setting expectations for the first 30 days is critical. Recovery begins with a single decision, followed by consistent action. The first week focuses entirely on stabilization—completing medical detox in a supervised environment where withdrawal symptoms are managed safely. This foundation allows the body to begin healing while the mind prepares for deeper work ahead.
Weeks two and three introduce structure through evidence-based therapies like CBT and DBT, combined with movement-based programming. Boxing sessions, hiking excursions, and ice bath therapy help restore neurochemical balance while building physical resilience. Group therapy creates accountability among peers who understand the journey firsthand, fostering a true sense of brotherhood.
By week four, men transition into developing sustainable routines. This includes identifying triggers, practicing coping strategies learned in individual therapy, and establishing connections within their support network. This solution fits men who are preparing to continue through intensive outpatient programming or transition to sober living, shifting the focus toward long-term integration.
Men's-only facilities across Tennessee continue this momentum through structured outpatient support and sober living environments designed to sustain what these first 30 days created.
The initial month following discharge from a residential facility is a decisive period for stabilizing progress and minimizing relapse risk. Data indicates that men who commit to a structured routine, maintain involvement in peer support, and continue movement-based or wellness activities are significantly more likely to remain engaged in recovery and transition successfully into outpatient or community supports2.
Prioritize this when your client benefits from clear goals and regular tracking. Daily movement, such as hiking or boxing, can reinforce mood regulation, while mindfulness helps manage stress and triggers. Communication with a support network and proactive participation in aftercare services are directly linked to higher rates of treatment completion and long-term recovery2. You can press Ctrl + D to bookmark these guidelines for your next client consultation.
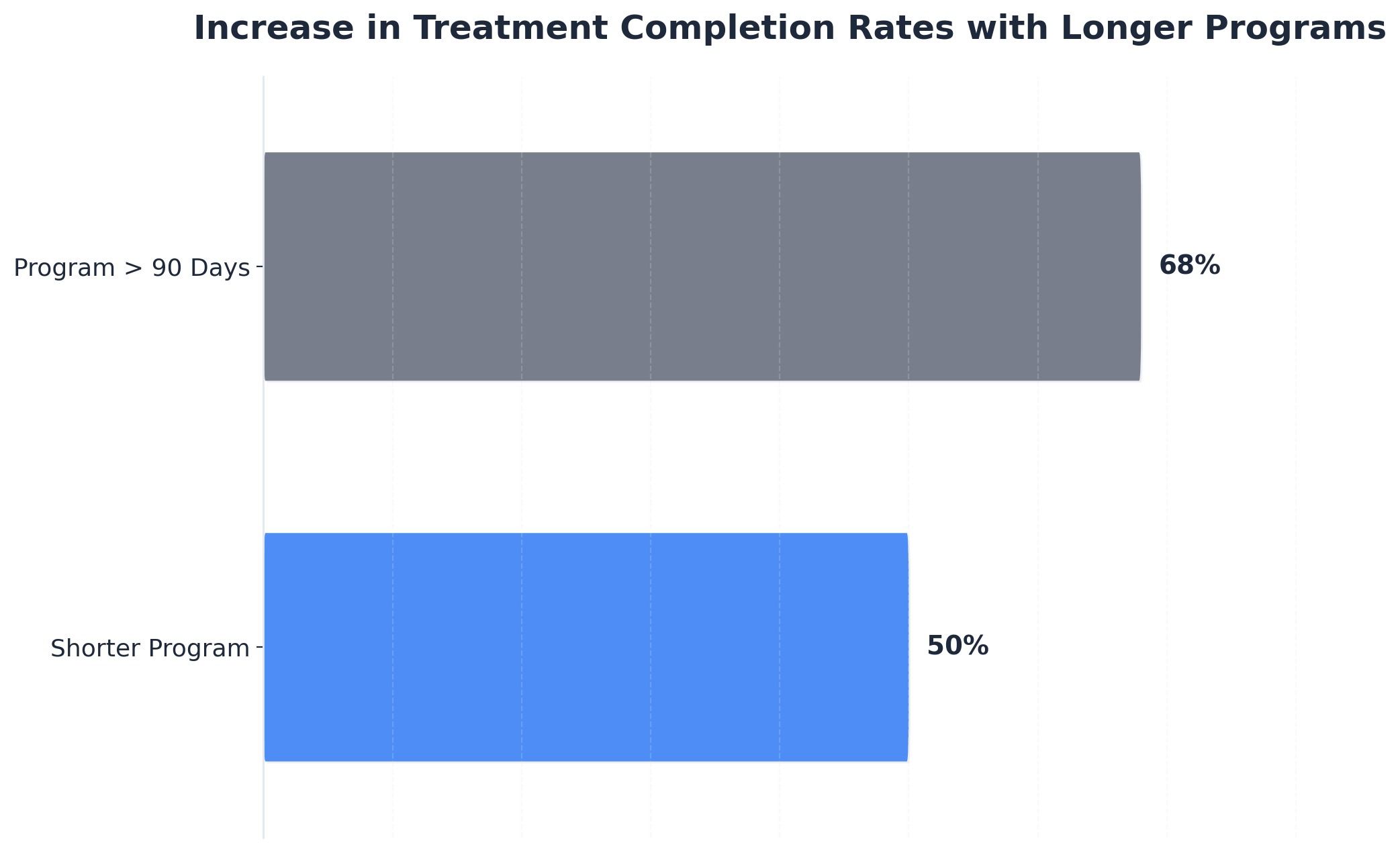
If 30 days in a short term drug rehab setting isn’t enough for medical stabilization or lasting behavioral change, clinical teams typically recommend a seamless transition into extended residential care or intensive outpatient programming. Research demonstrates that treatment completion rates increase from 50% to 68% when individuals engage in programs exceeding 90 days, provided that aftercare and support services remain robust 5. This solution fits men experiencing persistent cravings, severe withdrawal symptoms, or complex co-occurring mental health challenges that require a longer therapeutic window. Ongoing clinical assessment, family input, and peer support help identify who benefits most from a step-up in care intensity.
Insurance often shapes the length of stay in short term drug rehab, sometimes limiting access to extended residential treatment even when clinical teams recommend additional time. Many insurance plans authorize a standard 28-30 day stay, citing evidence that this duration addresses acute stabilization and withdrawal management for many men. However, peer-reviewed studies highlight that longer treatment—exceeding 90 days—yields higher completion rates and improved outcomes, especially when robust aftercare is involved 5. This approach works best when organizations advocate proactively for coverage extensions, using documented clinical progress and ongoing medical necessity. Navigating insurance constraints requires early, ongoing communication between clinicians, insurers, and families to minimize disruption and support the safest possible care transition.
Short-term drug rehab can be beneficial for men with a severe trauma history, but its effectiveness hinges on the program's ability to address both acute stabilization and trauma-informed care needs. Evidence indicates that individuals with high trauma severity often require extended treatment duration and integrated psychiatric support to achieve sustained recovery, as traditional short-term models may not provide sufficient time for processing complex trauma 10. This approach is most appropriate when the short-term setting includes robust trauma screening, individualized care planning, and a clear pathway to longer-term therapy or step-down programming. For men with active PTSD symptoms or significant trauma-related distress, consider prioritizing programs with strong clinical integration and aftercare linkage.
Completing a short term drug rehab program means meeting the requirements of the structured treatment—such as attendance, participation, and planned discharge—usually within a 28- to 30-day window. Achieving sustained recovery, however, extends well beyond program completion and involves ongoing abstinence, engagement in aftercare, development of coping skills, and healthy reintegration into daily life. Research shows that while program completion is a positive milestone, long-term recovery outcomes depend on continued involvement in outpatient care, peer support, and relapse prevention strategies 2. This distinction is crucial for professionals guiding men through early stabilization toward meaningful, durable change.
Medication-assisted treatment (MAT), which includes medications like buprenorphine, methadone, or naltrexone, can significantly enhance the effectiveness of short term drug rehab—especially for men with opioid use disorder. Research shows that individuals started on MAT during residential care have 20–30% better treatment outcomes and are more likely to stay engaged in follow-up care after discharge 8. This approach works best when MAT is integrated early, paired with counseling and structured aftercare planning. For programs serving men at high risk of relapse or severe withdrawal, initiating MAT within a short-term rehab setting directly supports stabilization and smoother transitions to outpatient MAT management.
Employment stability is a key factor in determining the appropriate length of stay in a short term drug rehab program. Men with secure jobs and supportive workplaces may be candidates for 28-30 day programs, as returning to work promptly can reinforce accountability and structure—both protective factors for sustained recovery. On the other hand, those facing unemployment or job instability often benefit from extended residential or step-down care, which allows more time to build coping skills and address underlying barriers to re-employment. Research highlights that employment status and supportive social structures predict stronger recovery outcomes, while unstable employment may signal a need for longer or more intensive programming 10.
Telehealth can play a pivotal role in extending the benefits of short term drug rehab by making ongoing therapy, peer support, and psychiatric check-ins accessible after discharge. Virtual appointments reduce barriers linked to transportation, work schedules, or rural location, allowing men to maintain continuity with their clinical team and support network. Research highlights that integrating telehealth into aftercare planning improves treatment retention and supports smoother transitions to outpatient care for graduates of residential programs 2. This approach works well for men who need flexibility, those returning to demanding jobs, or individuals in areas with limited in-person treatment options. Telehealth also enables early intervention if challenges or relapse risks emerge between scheduled in-person visits.
April 13, 2026

April 15, 2026

April 15, 2026