


April 13, 2026
What Does Mental Health Support for Men Look Like?
Explore effective men’s mental health support through integrated care, movement therapies, and peer-driven recovery by Trifecta Healthcare Institute.
Read More
Explore effective alumni services for men in crisis with peer support, mentorship, and movement programs to sustain recovery at Trifecta Healthcare Institute.
Start Your Journey NowWritten and reviewed by the clinical team at Trifecta Healthcare Institute, a men’s-only treatment center in Tennessee specializing in substance use, mental health, and dual diagnosis care.
You already know that walking out of treatment isn't walking into "recovered." For professionals navigating high-stress careers, finding effective alumni services for man in crisis is the bridge between intensive care and sustainable, long-term success. Discharge represents a transition point, not a finish line. The question isn't whether recovery continues afterward; it's how the foundation built during intensive treatment translates into sustainable momentum when structure dissolves and real life resumes.
"The neurological reality alone demands ongoing engagement. While medical detox clears the acute crisis, the brain's recalibration process extends months beyond discharge."
Men leaving a Nashville rehab or Knoxville rehab for men enter a critical window where reward pathways, stress responses, and emotional regulation systems remain vulnerable. At Trifecta Healthcare Institute, the movement-based programming introduced during treatment—boxing, jiu-jitsu, ice baths—isn't recreational filler; it's establishing neurochemical patterns that require consistent reinforcement. These activities become tools you carry forward, but only if the transition includes structured continuation rather than abrupt cessation.
The environmental shift presents the more visible challenge. You move from 24/7 accountability into settings saturated with previous triggers, relationship dynamics, and stressors that originally contributed to substance use patterns. Professional responsibilities resume immediately, and family expectations return in full force. The protective structure of residential treatment evaporates overnight, demanding evolved coping mechanisms and ongoing skill development that extends far beyond initial program completion.
Co-occurring mental health conditions follow their own timeline as well. Anxiety, depression, and trauma responses don't resolve within 30 or 60 days of treatment. While Trifecta does not offer primary mental healthcare, we provide essential co-occurring mental health treatment alongside substance use disorder (SUD) support. This dual diagnosis framework requires sustained therapeutic intervention and consistent monitoring to prevent symptom escalation that could undermine your sobriety.
The brotherhood dimension proves equally critical to long-term outcomes. The peer accountability and authentic connection men develop during treatment at Trifecta's facilities create a support network that rivals clinical interventions in effectiveness. These relationships require intentional nurturing through alumni engagement, ongoing group connections, and structured opportunities to maintain the bonds formed during intensive phases. You need time to rebuild family trust and establish healthy relationships beyond treatment, and the brotherhood established during care provides the scaffolding for that broader social reconstruction.
Physical restoration follows a similar trajectory. The movement-based activities that begin during treatment establish patterns for stress management, emotional regulation, and neurochemical balance that must continue indefinitely. The habits formed during intensive treatment need reinforcement and evolution as you progress through different recovery stages. This is why Trifecta's approach integrates these activities as core therapeutic tools rather than amenities—they're designed for portability into life after discharge, creating continuity between structured care and independent recovery.
Solution 1: Brotherhood Accountability Frameworks
Brotherhood accountability frameworks have become a cornerstone of aftercare, especially in Tennessee’s men-focused recovery landscape. These frameworks intentionally foster a sense of responsibility, peer connection, and shared purpose—critical ingredients for sustained engagement after discharge. Instead of relying solely on clinician oversight, brotherhood models position peers as daily accountability partners, supporting each other through regular check-ins, group meetings, and activity-based commitments.
How it works: You participate in structured routines—such as weekly group challenges, team-based physical activities, or skill-building workshops—where progress and setbacks are openly discussed within a trusted circle. This atmosphere of mutual accountability not only strengthens commitment but also activates neurobiological reward pathways, serving as a healthy alternative to substance-seeking behaviors.3
Comparison: Brotherhood Framework vs. Traditional Aftercare
When implemented alongside clinical guidance, brotherhood accountability frameworks provide a practical, evidence-backed foundation for your ongoing recovery, reinforcing the personal and community bonds essential in long-term healing. Next, we’ll examine how peer recovery specialists put these frameworks into action and extend their impact.7
Solution 2: Peer Recovery Specialists in Action
Peer recovery specialists (PRS) are individuals with lived experience of substance use disorder and sustained recovery who are professionally trained to support others. PRS extend the reach of clinical teams, providing mentorship, advocacy, and real-time guidance as you navigate post-discharge obstacles. Their credibility stems from personal understanding of relapse triggers, isolation, and the unique pressures faced by professional men in recovery.
How it works: PRS are embedded within alumni support networks, offering 1:1 check-ins, crisis navigation, and group facilitation. They model resilience, share practical coping strategies, and help bridge gaps between clinical care and real-world application. This lived-experience support has been shown to improve trust, reduce stigma, and sustain engagement—especially during high-risk transition periods.8
Impact of Peer Recovery Specialists on Outcomes
Peer recovery specialists deliver a powerful, evidence-backed layer of support, turning lived experience into a source of hope and practical guidance. Next, we’ll explore how movement-based programming further reinforces recovery for men after discharge.8
Solution 3: Neurobiological Mechanisms of Activity
Movement-based alumni programming taps into powerful neurobiological pathways that directly support recovery. Regular physical activity—such as boxing, hiking, or cold immersion—restores dopamine balance, reduces stress reactivity, and promotes neuroplasticity, all of which are often disrupted by long-term substance use. By harnessing these mechanisms, these programs offer more than routine fitness; they provide a biochemical foundation for resilience and relapse prevention.6
How it works: Exercise stimulates the release of brain-derived neurotrophic factor (BDNF), which repairs and strengthens neural circuits damaged by addiction. Physical challenge also triggers endorphin and dopamine production, replacing the neurochemical spikes once associated with substance use. Ice baths and high-intensity training activate the parasympathetic nervous system, promoting calm and emotional regulation—a critical counter to stress-induced cravings.6
When tracking your recovery metrics, you might log your daily ice bath duration into your recovery-tracker app and hit Save to monitor your dopamine baseline over time.
Neurobiological Impact of Movement-Based Care
Understanding these mechanisms sets the stage for examining how structured physical engagement models put neuroscience into practice and drive better recovery outcomes.
Solution 4: Structured Physical Engagement Models
Structured physical engagement models move beyond casual exercise, embedding purposeful movement into the core of aftercare programming. These models—such as scheduled boxing sessions, group hikes, or martial arts classes—offer a consistent, action-oriented framework that keeps you actively involved and accountable. Unlike ad hoc fitness, structured engagement relies on routine, peer participation, and professional facilitation to ensure ongoing motivation and safe progression.
How it works: Alumni commit to a regular schedule of physical activities that are both challenging and rewarding. Participation is tracked and often paired with group discussion or reflection to strengthen bonds and reinforce healthy behavioral patterns. These programs are intentionally designed to activate the reward circuitry in the brain, providing a biochemical substitute for the highs once sought through substance use.6
// Example Weekly Alumni Engagement Metric Tracking Structured vs. Unstructured Physical Engagement
Structured physical engagement offers a reliable channel to foster routine, connection, and healthy neurochemical reinforcement—key drivers in lasting recovery. Next, we examine how integrated co-occurring care in aftercare addresses trauma and mental health needs for men post-rehab.6
Solution 5: Trauma-Informed Alumni Services
Trauma-informed alumni services have become a vital component of aftercare for men navigating substance use disorder and co-occurring mental health challenges. With 60-80% of individuals in addiction treatment reporting trauma histories, alumni programming that actively recognizes, addresses, and supports trauma recovery is no longer optional—it’s a clinical necessity. While Trifecta does not offer primary mental healthcare, we specialize in co-occurring mental health treatment alongside SUD support. These services typically integrate evidence-based approaches such as EMDR, DBT, and movement-based therapies within a peer-supported framework, fostering both safety and accountability as you transition out of intensive care.9
How it works: Trauma-informed services emphasize psychological and physical safety, offer regular check-ins with trauma-trained staff or peers, and provide access to ongoing groups where trauma, stress, and triggers can be processed in a supportive environment. Many programs also incorporate somatic and experiential modalities, acknowledging that trauma is stored in the body as well as the mind.
Pros and Cons of Trauma-Informed Alumni Services
Trauma-informed alumni services are especially effective when paired with other supports, forming a foundation for resilience and reducing relapse risk during post-rehab reintegration. The next section will focus on how alumni programming facilitates community reintegration and vocational growth for men post-discharge.9
Solution 6: Community Reintegration and Vocational Support
Effective aftercare recognizes that sustainable recovery relies on more than just abstinence—it requires meaningful social and vocational re-engagement. Structured community integration and vocational support are now widely adopted best practices, helping you develop purpose, stability, and a sense of belonging after discharge. Research reveals that alumni who participate in employment support and community activities have a 72% sustained abstinence rate and 60% employment rate, compared to just 38% and 25% for those without such supports.10
How it works: Alumni programs may provide job coaching, resume workshops, interview preparation, and direct connections to local employers. Community reintegration often includes volunteering, peer-led service projects, or group outings that build social skills and expand support networks. These activities foster confidence, accountability, and resilience against relapse triggers like isolation or unemployment.
Pros and Cons of Vocational Support
Programs that prioritize both community and vocational growth empower you to reclaim roles as providers, leaders, and engaged citizens—core drivers of lasting recovery. Next, the FAQ section will address practical questions about implementing and measuring successful alumni programming.10

Addressing these challenges requires a comprehensive approach that bridges the gap between intensive treatment and independent living. At Trifecta Healthcare Institute's Nashville and Knoxville locations, the continuum model provides graduated support designed specifically for this critical transition period when relapse risk peaks.
A typical progression through Trifecta's continuum begins with medical detox, followed by a partial hospitalization program (PHP) where men engage in 6+ hours daily of therapeutic programming—including CBT, DBT, and trauma-focused therapies—while beginning movement-based activities like boxing and jiu-jitsu. As stability increases, you transition to intensive outpatient programming (IOP) (3-4 hours daily, 3-5 days weekly), maintaining clinical accountability while gradually increasing independence. Throughout this progression, structured sober living environments in both Nashville and Knoxville provide peer support, routine, and real-world practice of recovery skills. This graduated approach allows you to build confidence and coping mechanisms incrementally rather than facing an abrupt transition from 24/7 care to complete independence.
Tennessee's recovery landscape increasingly recognizes that physical engagement accelerates neurological healing—a principle central to Trifecta's programming. Movement-based therapies, from boxing and jiu-jitsu to outdoor adventure activities like hiking Tennessee's trails and white-water rafting, help restore dopamine regulation disrupted by substance use. These approaches prove particularly effective for men who struggle with traditional talk therapy formats, offering tangible outlets for processing trauma while rebuilding physical and mental resilience.
The brotherhood model distinguishes Trifecta's approach by creating lasting accountability networks that extend well beyond clinical discharge. Men who establish genuine peer connections during treatment—reinforced through shared physical challenges and men-only group dynamics—maintain these relationships through alumni services and ongoing community activities. This sustained brotherhood accountability, combined with continued engagement in movement-based practices, transforms recovery from a finite treatment episode into a lifelong framework for healing and growth.
When you or someone you love are ready to begin healing—mind, body, and spirit—connect with Trifecta Healthcare Institute. We help men thrive in and out of treatment.
Insurance reimbursement for extended alumni services beyond initial treatment discharge varies widely by payer and state. Medicaid and some commercial insurers now support alumni services for man in crisis through value-based care models, especially where aftercare is integrated with co-occurring mental health support. Covered services may include peer coaching, movement-based activities, and vocational support if they are documented as medically necessary. However, limitations remain: reimbursement often excludes purely social programming or alumni events not tied to clinical outcomes. Providers must carefully document ongoing medical need and functional progress. As of 2024, 32 states fund integrated alumni aftercare through Medicaid waivers, but coverage policies remain inconsistent.4
To demonstrate the effectiveness of alumni services for man in crisis, treatment centers should track metrics that reflect both clinical outcomes and engagement quality. Core indicators include sustained abstinence rates at 12 and 24 months, alumni engagement/retention over time, employment and community integration rates, and reductions in relapse and acute care utilization. Peer-reviewed research shows programs tracking these outcomes—especially when disaggregated by peer support involvement—can report up to 72% sustained abstinence and 60% employment for alumni in structured models, compared to 38% and 25% in non-supported groups. These data-driven metrics help stakeholders assess impact, guide resource allocation, and support continuous improvement.10
Alumni services for man in crisis are designed to promote independence, but there is a risk that overly intensive or indefinite programming may inadvertently create dependency on external support rather than fostering self-sufficiency. This risk is heightened when alumni services provide all decision-making structure or social connection, potentially discouraging men from developing their own coping strategies and community ties. However, research shows that structured, time-bound alumni models—especially those with clear goals and gradual step-downs in support—are associated with higher autonomy and better long-term outcomes compared to open-ended or highly paternalistic programs. The key is balancing accountability and connection with opportunities for personal growth and self-directed recovery.5
Virtual alumni support has become a valuable option for professionals needing confidentiality, flexibility, and ongoing connection after discharge. Alumni services for man in crisis delivered online—such as secure video groups or encrypted messaging—can reduce barriers for men who are concerned about privacy or face logistical challenges attending in-person meetings. Virtual models increase access for rural or busy professionals and have demonstrated engagement rates comparable to, or sometimes exceeding, those of in-person formats, especially when anonymity and convenience are priorities. However, in-person programming still offers stronger peer bonding and accountability, which supports deeper relationships and more robust behavioral change. The optimal approach often blends both, giving professionals the autonomy to engage in ways that best support their recovery journey.3
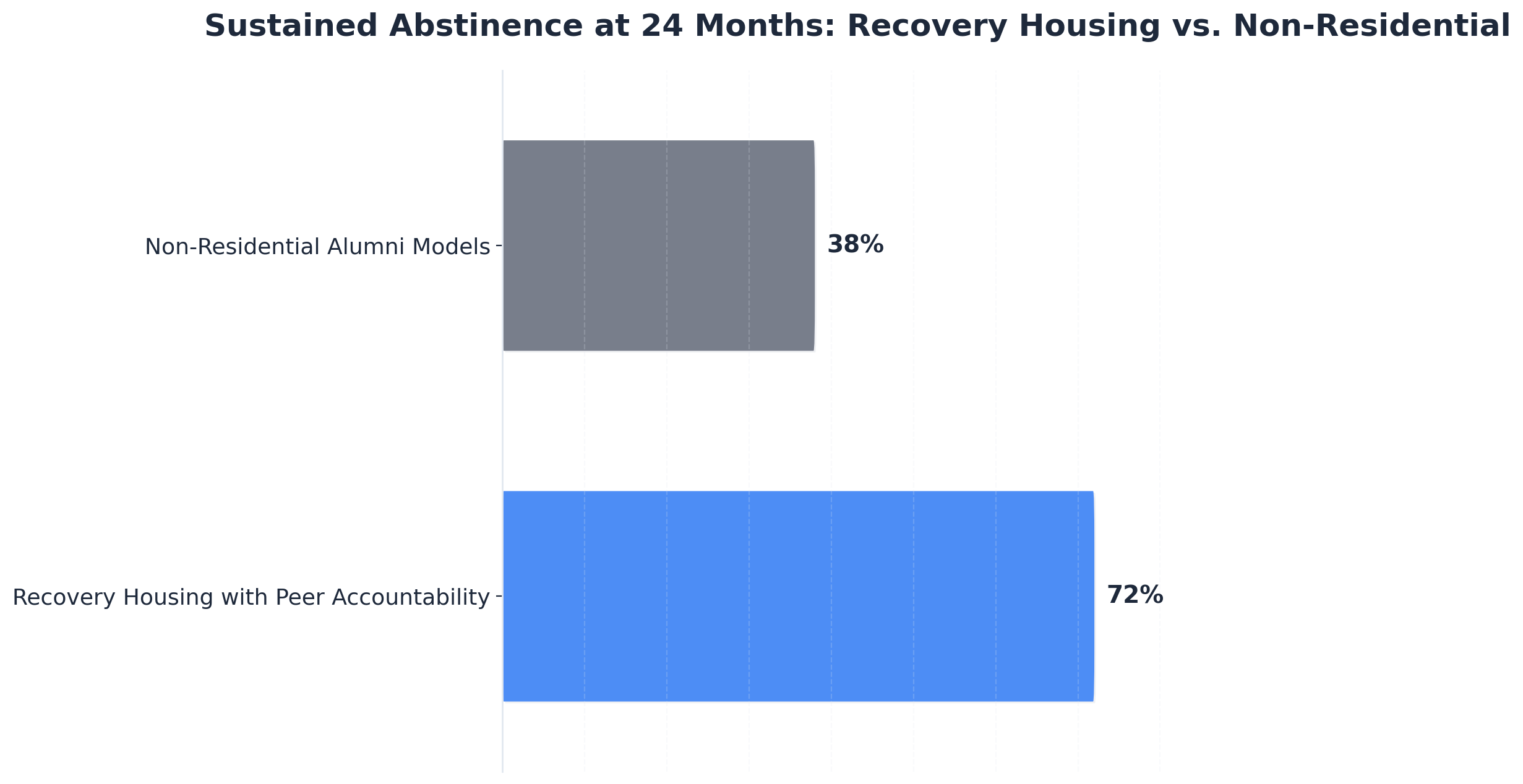
The optimal duration of structured alumni engagement for men in crisis appears to be 18–24 months post-discharge. Research shows that alumni services for man in crisis delivered within this window are linked to the highest sustained abstinence rates—upwards of 72% in recovery housing models—while minimizing the risk of fostering dependency. During this time, programming should gradually shift from high-intensity peer and clinical support to more autonomous, goal-oriented activities, allowing men to build confidence in their own coping strategies. Open-ended, indefinite alumni support can sometimes undermine self-sufficiency, so a time-bound, step-down approach is recommended by leading experts. Ongoing peer connection beyond 24 months remains beneficial but should prioritize empowerment and self-direction.5
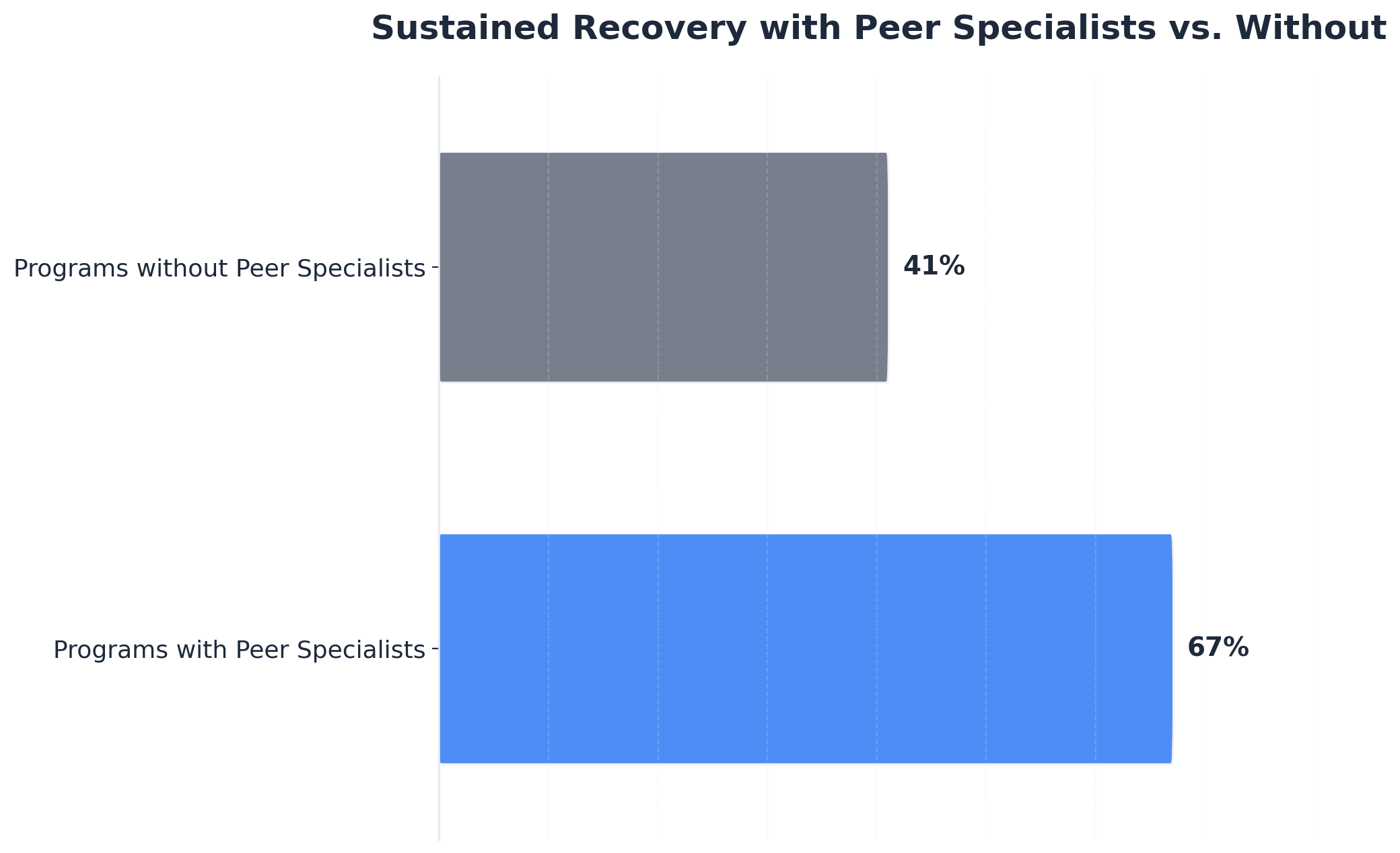
Peer recovery specialists with lived experience often achieve outcomes in alumni services for man in crisis that rival or surpass those of licensed clinicians, especially regarding trust, engagement, and sustained recovery. Programs staffed by peer recovery specialists report 67% sustained recovery rates, compared to 41% in programs without them. Their lived experience allows for relatable guidance and real-time support, fostering deeper peer connections. Licensed clinicians bring advanced clinical expertise and can address complex psychiatric needs, but may not always establish the same level of peer credibility. Many centers now blend both roles to maximize engagement, accountability, and clinical safety in alumni programming.8
April 13, 2026

April 15, 2026

April 15, 2026